HealthTech Startups Solving Indian Infrastructure Gaps
July 1, 2026 by Harshit Gupta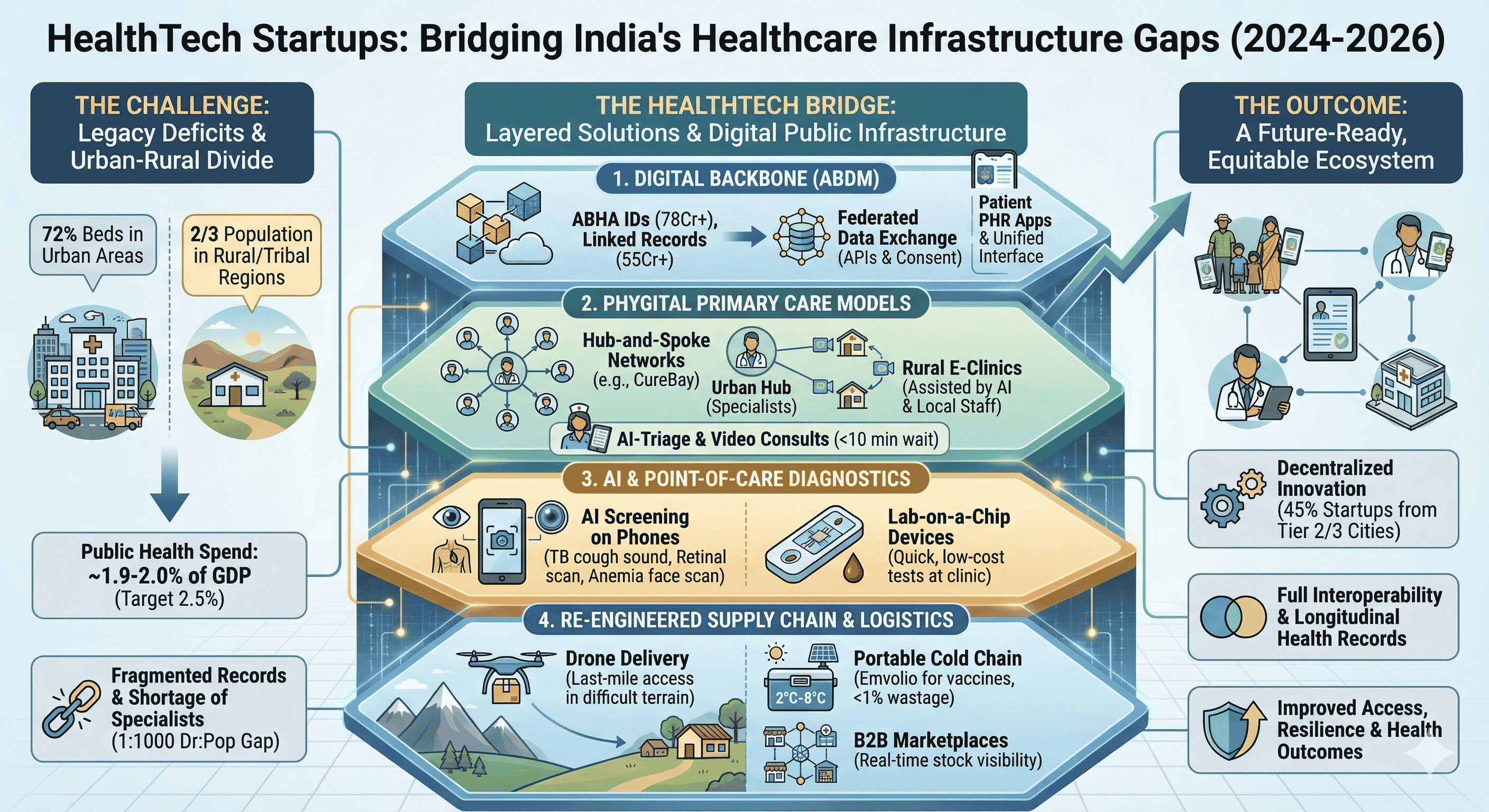
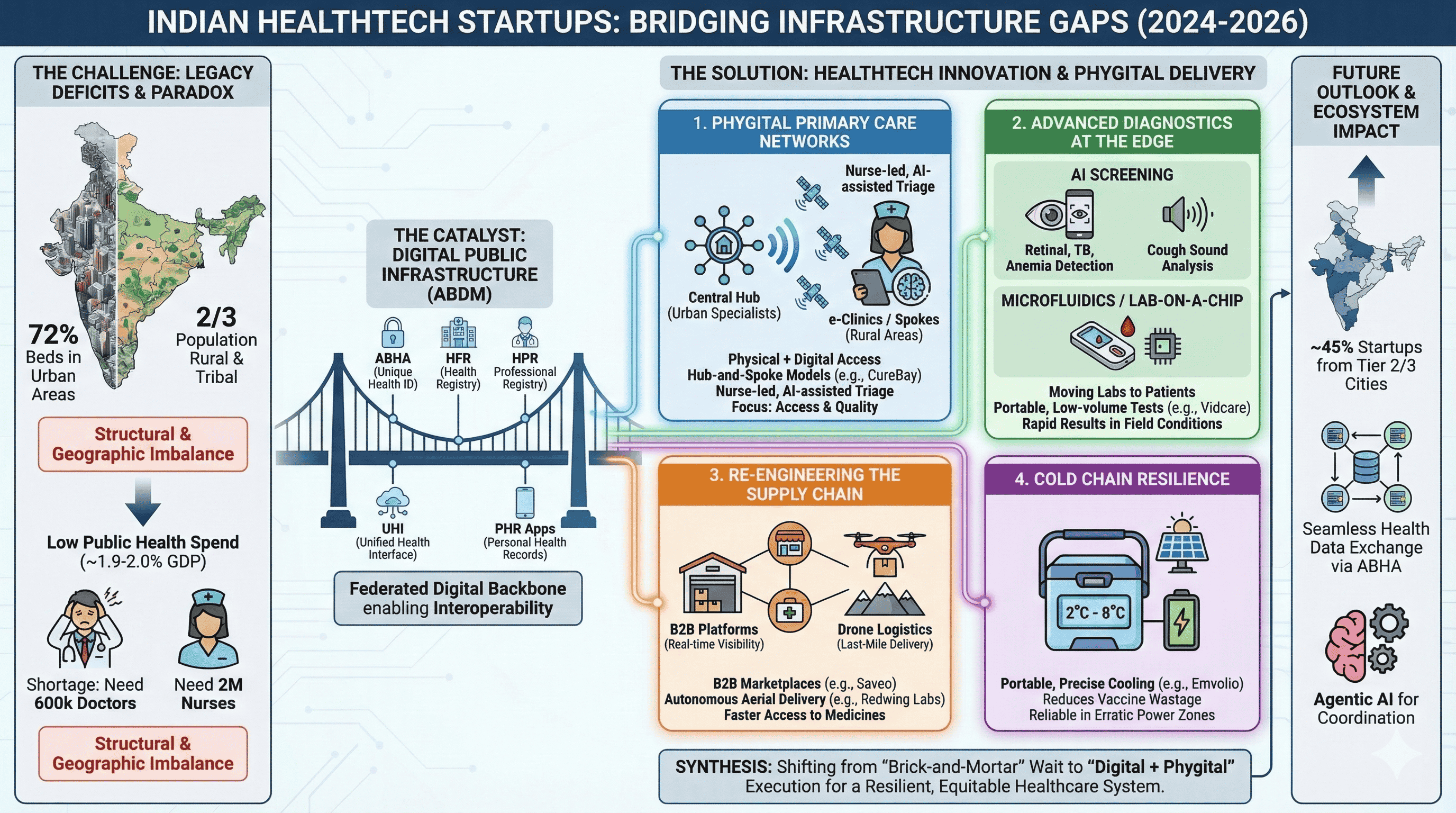
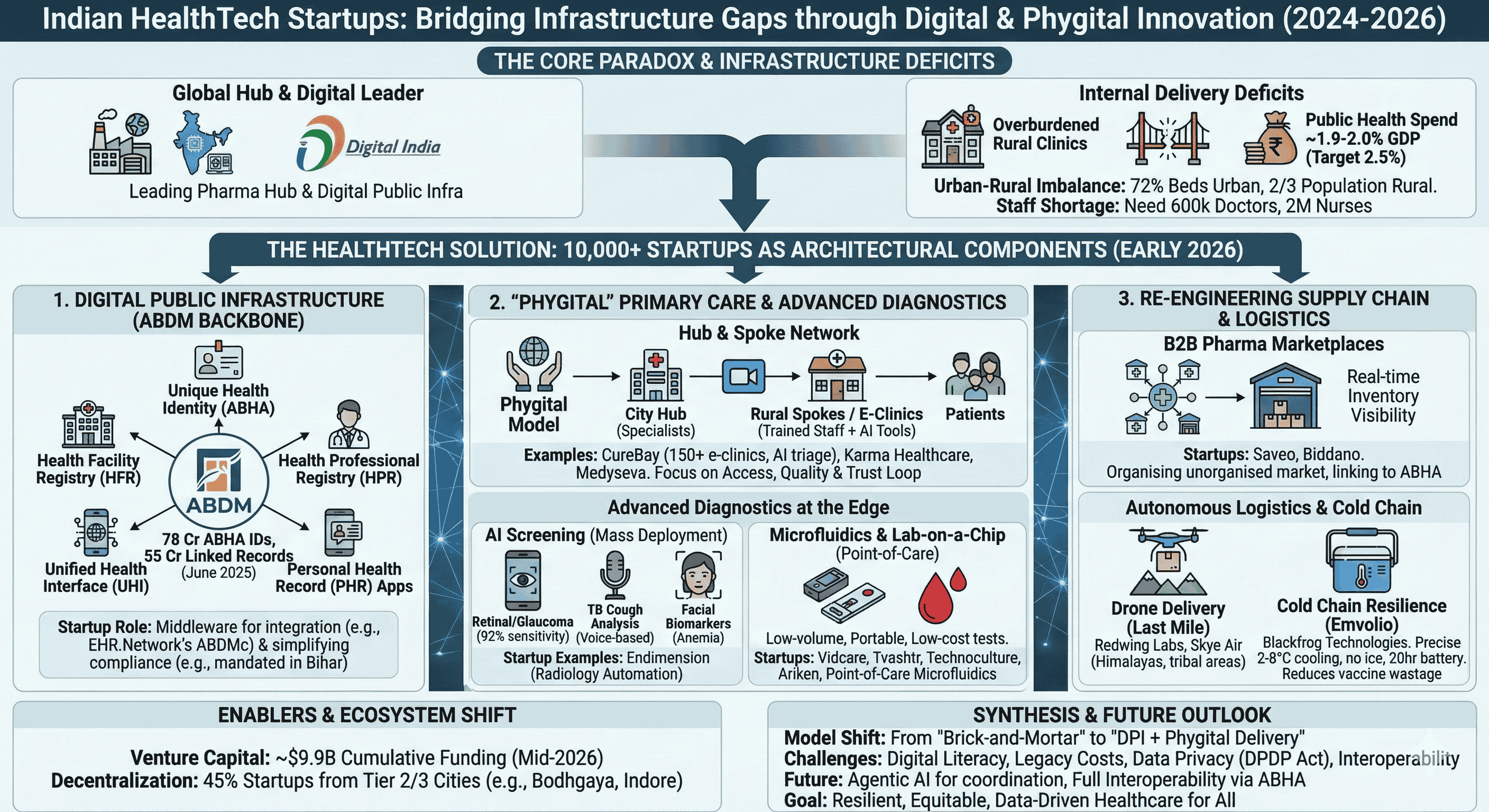
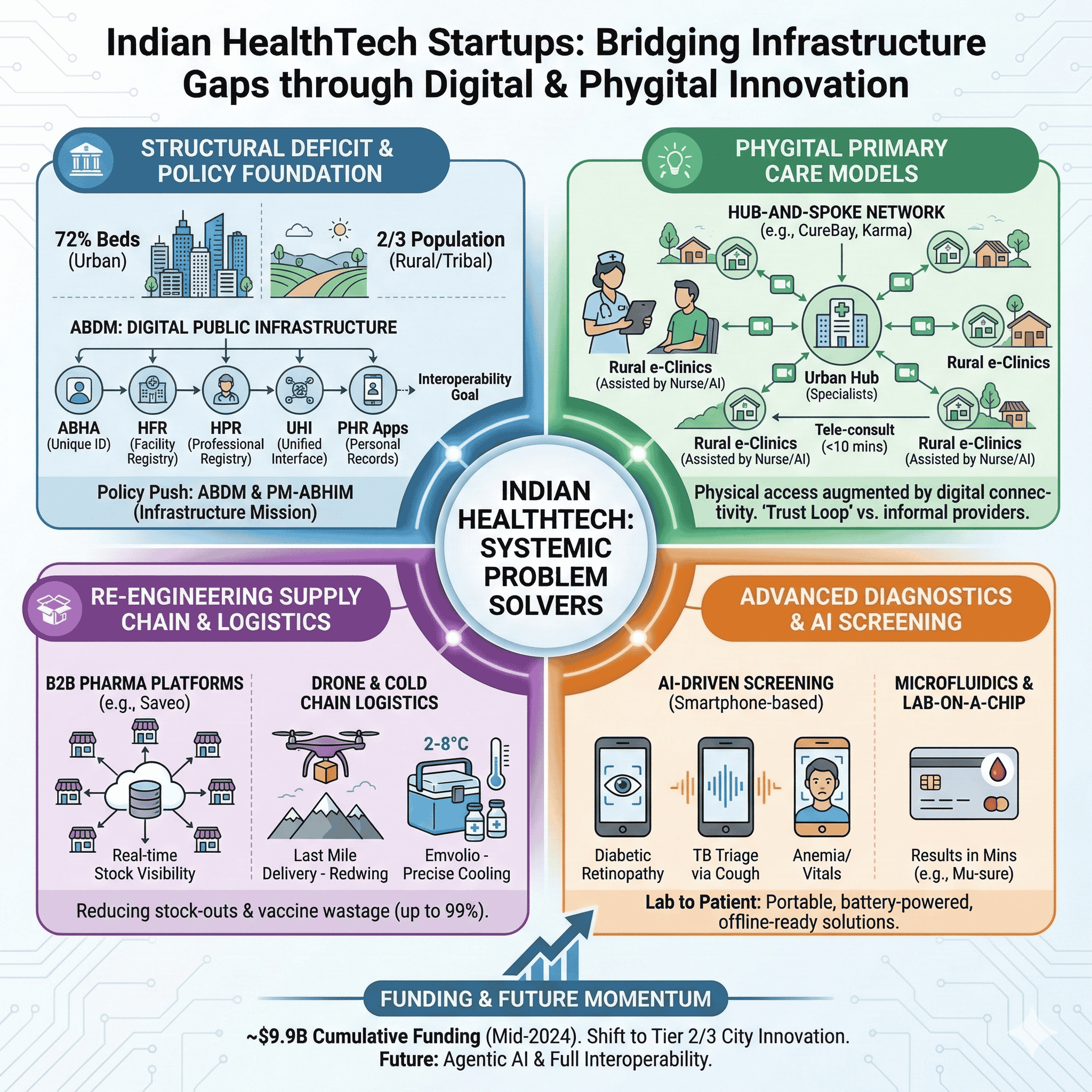
The structural trajectory of the Indian healthcare system is currently defined by a profound paradox. While the nation asserts its position as a global pharmaceutical hub and a leader in digital public infrastructure, the internal delivery mechanisms for primary and secondary care continue to grapple with legacy deficits that impede universal access. The aspiration to increase public health expenditure to 2.5% of Gross Domestic Product (GDP) by 2025 remains a challenging target, as current allocations hover around 1.9% to 2.0% of the total budget. Within this high-stakes environment, the Indian HealthTech sector—comprising over 10,000 active startups as of early 2026—has transitioned from being a peripheral provider of convenience-based apps to a core architectural component of the national health system. These ventures are systematically addressing infrastructure gaps through a layered approach: utilizing digital identity frameworks, deploying "phygital" (physical plus digital) care models, and re-engineering the medical supply chain through autonomous aerial and ground-based logistics.
The Structural Deficit and the National Policy Response
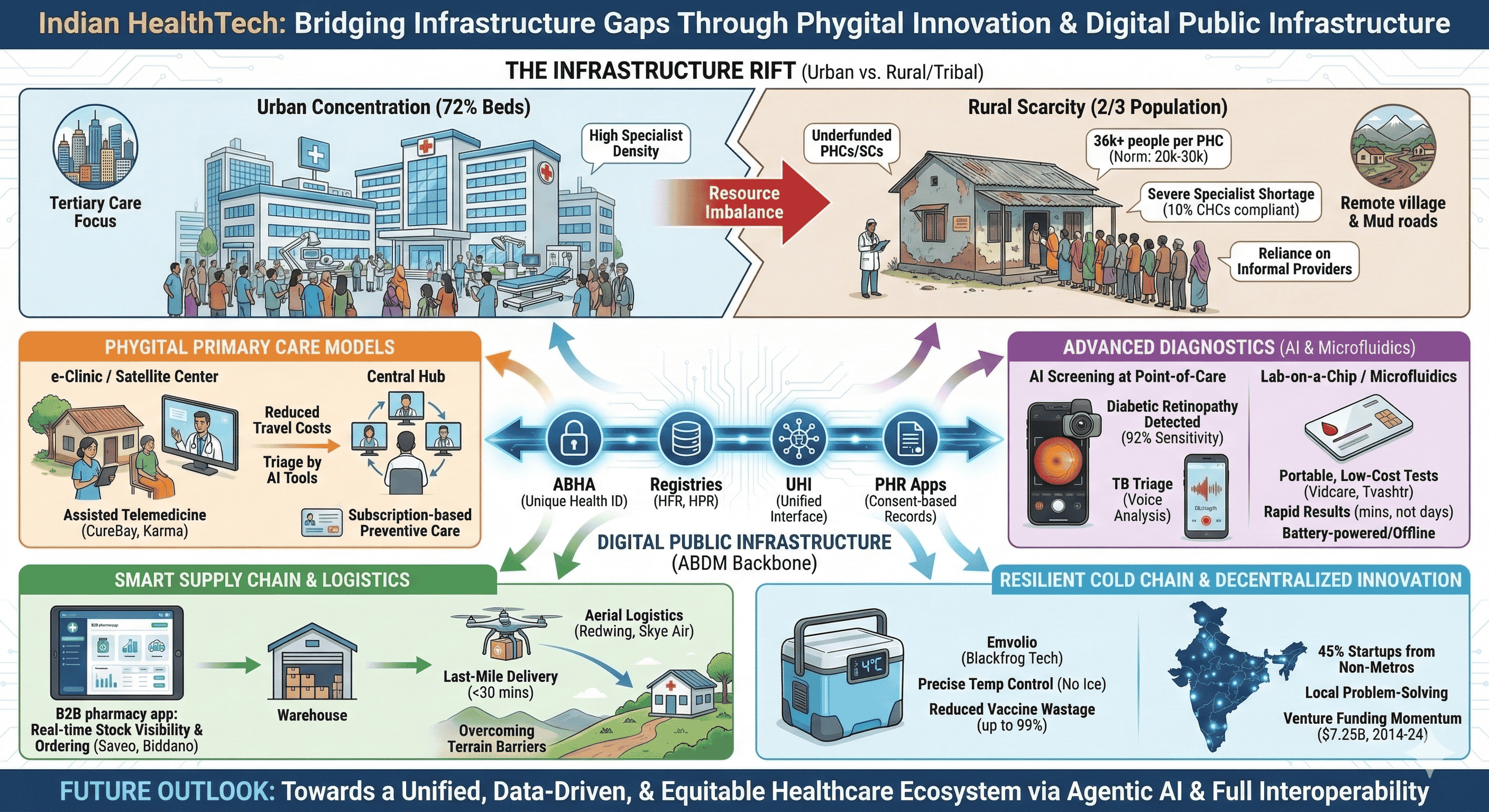
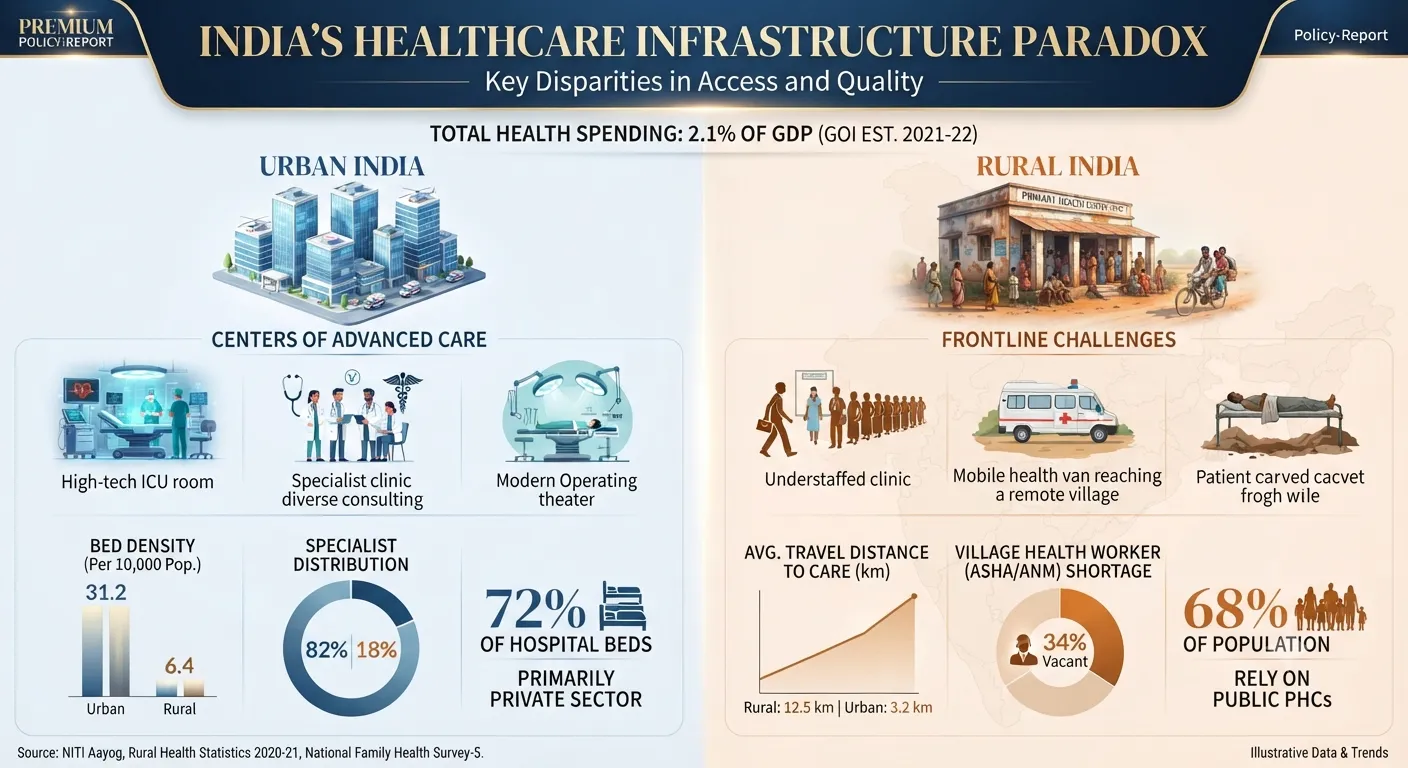
The fundamental challenge in Indian healthcare is not merely a lack of capital, but a severe geographic and tiered imbalance in resource distribution. Approximately 72% of all hospital beds in the country are concentrated in urban areas, yet nearly two-thirds of the population resides in rural and tribal regions. This concentration of tertiary care has left the primary healthcare foundation—the Sub-Centres (SCs) and Primary Health Centres (PHCs)—structurally underfunded and overstretched. As of 2021-2022, a PHC typically caters to an average of 36,049 individuals, significantly exceeding the target norm of 20,000 to 30,000 persons.
The Union Budgets for the fiscal years 2024-25 and 2025-26 reflect a complex prioritization strategy. While the National Health Mission (NHM) remains the flagship program for rural health, its budgetary share has seen a declining trend in real terms over the last five years. Conversely, the government has intensified investment in the Pradhan Mantri Ayushman Bharat Health Infrastructure Mission (PM-ABHIM), which received ₹3,757 crore in 2024-25, a 63% increase aimed specifically at disease surveillance and strengthening primary care infrastructure.

Health Allocation Metric | 2023-24 (Revised Estimates) | 2024-25 (Budget Estimates) | 2025-26 (Projected) | Source |
Total Health Ministry Budget (₹ Cr) | 80,518 | 90,659 | 95,958 | |
National Health Mission (₹ Cr) | 31,551 | 36,000 | 37,227 | |
AB-PMJAY Insurance (₹ Cr) | 6,800 | 7,300 | 9,406 | |
PM-ABHIM Infrastructure (₹ Cr) | 2,300 | 3,757 | 4,200 | |
Health Expenditure as % of GDP | ~1.3% - 1.5% | ~1.6% - 1.8% | ~1.9% |
The systemic issues are further quantified by the acute shortage of human resources. India requires an estimated 600,000 additional doctors and two million more nurses to meet World Health Organization (WHO) recommendations of a 1:1,000 doctor-to-population ratio. In many states, the scarcity of specialists in Community Health Centres (CHCs) is alarming; as of the 2021-2022 reports, only 10% of CHCs had the required four specialists—surgeon, physician, obstetrician, and pediatrician—on-board. This vacuum has historically facilitated the rise of informal care providers or "quacks," who utilize their community proximity and established trust to provide treatment, often with the irrational and dangerous use of steroids and antibiotics.
Digital Public Infrastructure: The Ayushman Bharat Digital Mission (ABDM)
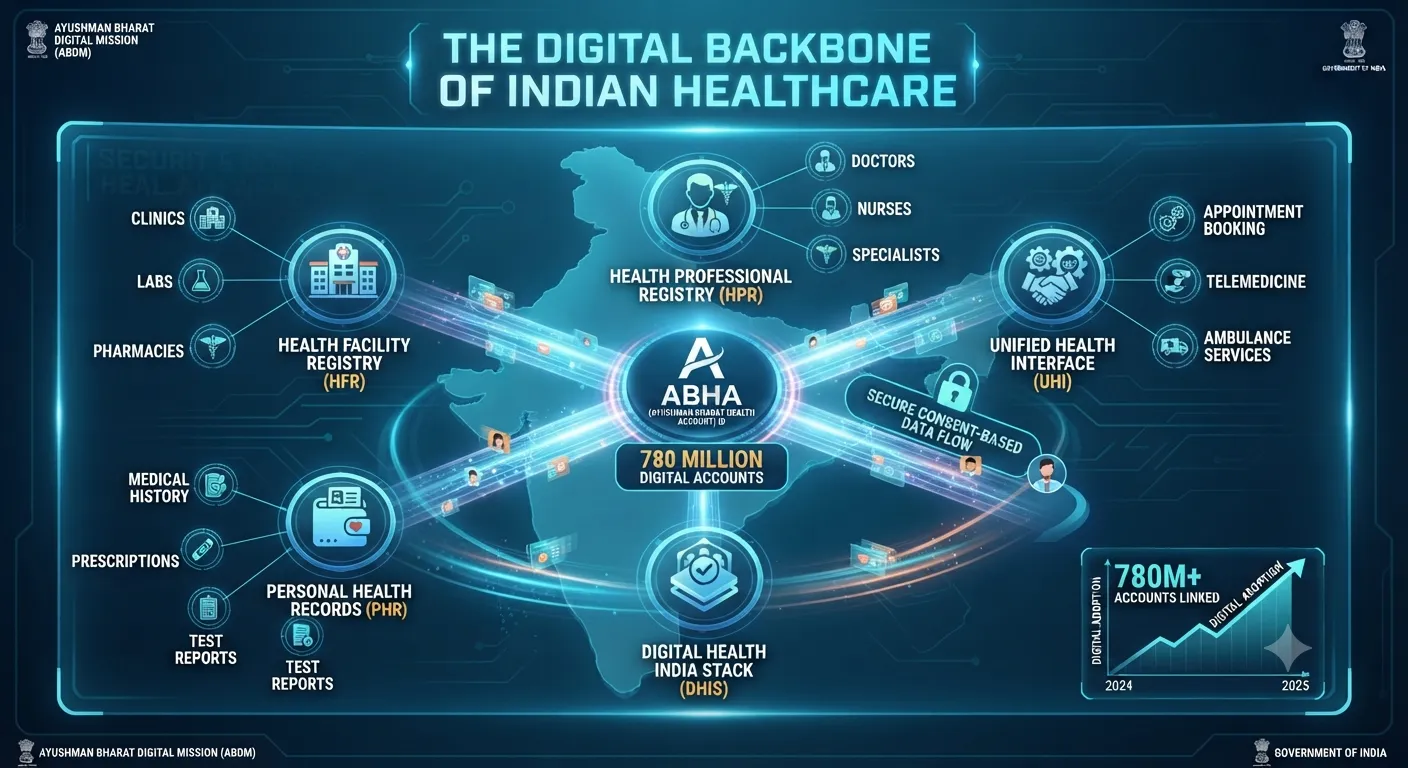
To address the fragmentation of patient records and the lack of interoperability between providers, the Government of India launched the Ayushman Bharat Digital Mission (ABDM) in 2021. By June 2025, the mission had reached a milestone of 78 crore Ayushman Bharat Health Accounts (ABHAs) and linked over 55 crore health records. The ABDM architecture is built on the principle of a federated digital infrastructure, where health data remains with the original custodians—hospitals, labs, or pharmacies—and is shared only upon patient consent.
This digital backbone provides five key structural innovations:
Unique Health Identity (ABHA): A 14-digit identifier that enables a longitudinal health record for every citizen.
Health Facility Registry (HFR): A comprehensive directory of public and private hospitals, clinics, and labs.
Health Professional Registry (HPR): A verified database of doctors and healthcare workers across both modern and traditional systems.
Unified Health Interface (UHI): An open network, similar to UPI for payments, that enables the discovery and booking of health services across different apps.
Personal Health Record (PHR) Apps: Consumer-facing interfaces that allow patients to view and share their medical history.
For HealthTech startups, ABDM serves as a transformative catalyst. By providing standardized APIs through its "Digital Sandbox," the government has enabled over 1,000 private companies to integrate their platforms into the national ecosystem. However, the transition from legacy, siloed IT systems to ABDM-compliant frameworks remains a significant barrier for many mid-sized and rural providers. The complexity of mapping data to FHIR (Fast Healthcare Interoperability Resources) standards and managing asynchronous workflows for consent-driven data exchange has created a market for specialized middleware.

Startups like EHR.Network, through its ABDM Connect (ABDMc) platform, have emerged to simplify this integration. By converting complex backend processes into easy-to-use synchronous APIs, these intermediaries help hospitals and health IT vendors achieve mandatory certifications for programs like the AB-PMJAY. In states like Bihar, compliance with ABDM workflows has been mandated for all private hospitals empanelled under the national insurance scheme, signifying a shift where digital adoption is no longer optional but a prerequisite for institutional revenue and operations.
State-wise Healthcare Infrastructure Readiness (PHC Level) | % of PHCs with 4+ Beds | % of PHCs Open 24 Hours | Source |
Odisha | 10% | Data N/A | |
Assam | 37% | Data N/A | |
Bihar | 41% | Data N/A | |
Maharashtra | Data N/A | 13% | |
West Bengal | Data N/A | 25% | |
Uttarakhand | Data N/A | 11% | |
Himachal Pradesh | Data N/A | 5% |
Reimagining Primary Care: Phygital Models and Rural Hub-and-Spoke Networks
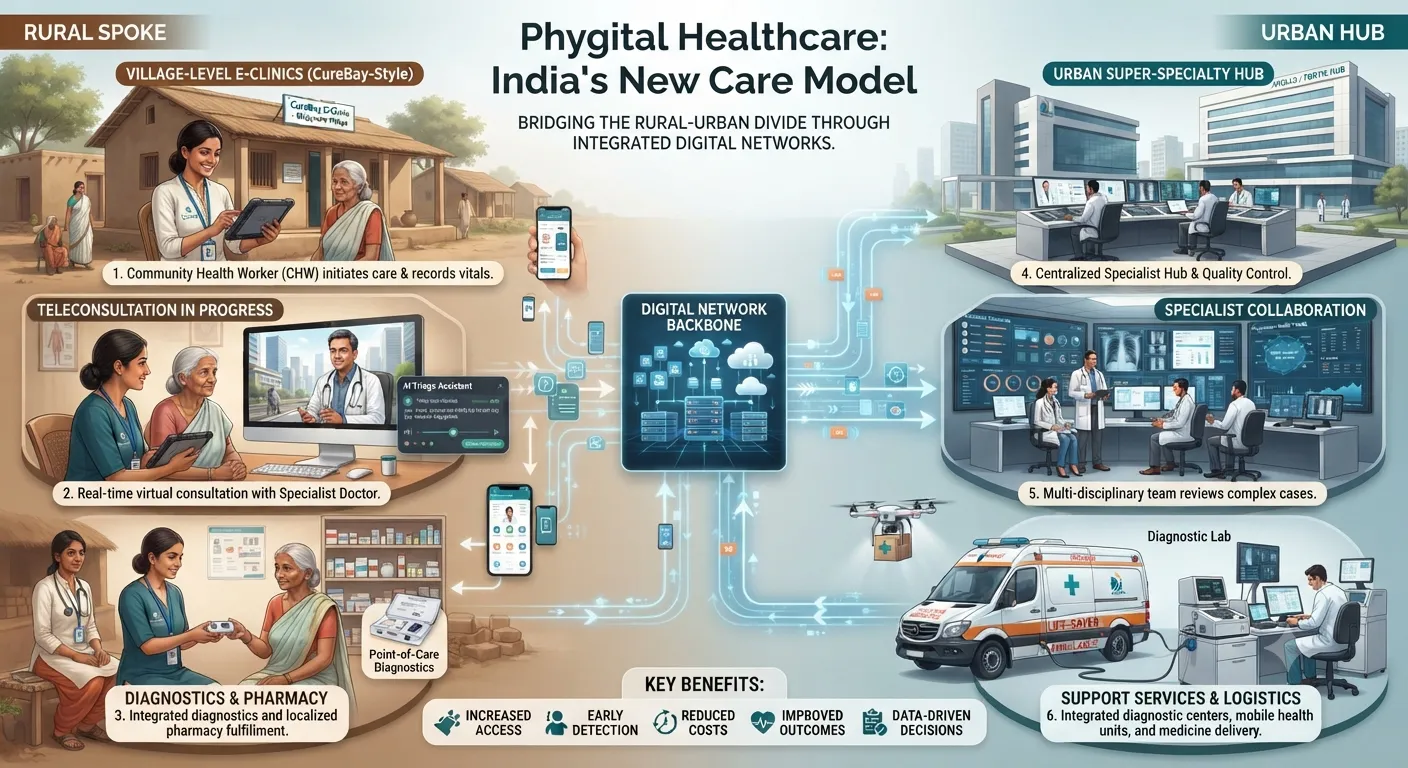
While urban HealthTech has focused on "convenience" (e.g., rapid medicine delivery in metros), the rural challenge is one of "access" and "quality." The pure-play telemedicine model often fails in remote regions due to low digital literacy, erratic internet connectivity, and the absence of local diagnostic support. In response, a cohort of "phygital" startups is building physical infrastructure augmented by digital connectivity.
CureBay, founded in 2021, represents a sophisticated execution of this hybrid model. Operating primarily in Odisha and Chhattisgarh, CureBay has established a three-tier fulfillment model comprising central hubs, spokes, and a network of satellite health centers or e-clinics. As of late 2025, the platform serves over 400,000 patients through more than 150 e-clinics, addressing nearly 80% of primary care needs in its operational areas. The e-clinics are staffed by trained health workers who use AI-driven tools like CareSathi to coordinate care, triage symptoms, and connect patients with city-based specialists via video consultation in under 10 minutes.
The economic logic of the CureBay model is predicated on the "circle" clinic network. By clustering clinics and sharing logistics and diagnostic partnerships, these operational clusters achieve break-even within 18 to 20 months. Furthermore, CureBay has successfully transitioned 100,000 rural individuals into a subscription-based preventive care program—a segment that urban providers have historically struggled to monetize. This suggests that rural populations are willing to pay for ethical, квалифицированный care (charging a standard consultation fee of ₹100) if it saves them the loss of daily wages and high travel costs associated with visiting urban tertiary centers.
Karma Primary Healthcare and Medyseva follow similar nurse-led, e-doctor clinic models. Karma Healthcare, founded in 2014, pioneered the use of trained nurses as the interface between rural patients and remote urban doctors. Medyseva, originating during the COVID-19 pandemic, focuses on "Medyseva Kendras" in Madhya Pradesh, providing an ideal mix of online consultation and offline diagnostic and ambulance support. These startups are effectively institutionalizing the informal care market, offering a formal, verified alternative to local quacks while building a "Trust Loop" through consistent, reliable outcomes.
Advanced Diagnostics: AI, Microfluidics, and Point-of-Care Testing
Diagnostic gaps are perhaps the most acute infrastructure failure in rural India. When a patient in a village requires a specialized test or a radiology interpretation, they often face a wait of several days and a multi-hour journey to a district headquarters. Indian HealthTech startups are solving this by moving the laboratory to the patient through artificial intelligence (AI) and microfluidics.
The AI Screening Revolution
In early 2026, the maturity of AI-driven screening became evident with the launch of several population-level tools designed for mass deployment by frontline workers like ASHA and ANMs. These tools prioritize high-burden conditions such as tuberculosis (TB), diabetic retinopathy, and anemia.
Retinal Screening: AI-powered smartphone adapters and algorithms are now capable of detecting diabetic retinopathy and glaucoma with over 92% sensitivity during community screenings. This technology allows for early intervention in a population where diabetes is increasingly prevalent.
TB Triage: Given India's record 26.17 lakh TB case notifications in 2024, screening efficiency is critical. Voice-based AI systems now analyze cough patterns and breathing sounds via basic smartphones to flag potential cases, achieving results comparable to high-end molecular tests like GeneXpert in field conditions.
Facial Biomarker Analysis: Contactless facial scan tools estimate anemia and vitamin deficiencies by analyzing subtle changes in skin tone and facial micro-expressions, delivering instant results with 85-90% lab-validated accuracy.
Radiology Automation: Endimension's radiology platform detects over 80 abnormalities across X-rays and CT scans, boosting radiologist efficiency by 4.2 times and reducing diagnostic turnaround times in over 1,000 facilities.
Microfluidics and Lab-on-a-Chip
Microfluidic technology enables complex biochemical tests to be performed using microliter volumes of fluids on compact devices, drastically reducing costs and resource requirements.
Startup | Location | Primary Innovation | Clinical Impact | Source |
Vidcare Innovations | Pune | Mu-sure disposable device | Credit card-sized device provides blood test results in 25 mins from 2 drops of blood. | |
Tvashtr Biotech | Jaipur | Host-molecule trapping chips | Portable kits for early detection of Alzheimer's and allergies using selective molecular trapping. | |
Technoculture Research | Bodhgaya | Pwomise molecular device | Integrates microfluidics with electrochemical electrodes to cut diagnostic costs by 10x. | |
Ariken Labs | Chennai | Capillarity & Acoustophoresis | Rare cell detection and blood plasma separation for monitoring vascular health and cancer. | |
Point-of-Care Microfluidics | Vellore | PDMS Lab-on-Chip | FET-based biosensors and sub-100 nm channels for DNA sequencing and medical diagnostics. |
These point-of-care (POC) solutions are designed with the "Indian context" in mind: they are often battery-powered, feature offline functionality for low-connectivity areas, and are cost-effective enough for small nursing homes and rural clinics.

Strengthening the Supply Chain: B2B Marketplaces and Aerial Logistics
The pharmaceutical supply chain in India suffers from high fragmentation and limited real-time visibility. Stock-outs at the chemist level often force patients to travel to larger cities to procure prescribed medicines. Startups are addressing this by creating structured B2B networks and utilizing autonomous drones for the "last mile."
B2B Pharma Platforms
Marketplaces like Saveo, Biddano, and Retailio aim to provide drugstores with visibility into distributor stocks. Saveo, headquartered in Bengaluru, operates an asset-light model that links orders to suppliers and dark stores, delivering to over 120 towns across South India. By providing an ERP system that helps pharmacies track their own inventory, Saveo enables small chemists to maintain a broader range of stocks without the financial burden of overstocking. Biddano uses AI technology to ensure that pharmacies can procure medicines within three hours of ordering, effectively organizing the offline pharmaceutical distribution network.
However, the sector has seen consolidation and volatility. While Saveo reached an annual revenue of ₹160 crore as of March 2025, other players have faced challenges with unit economics and aggressive expansion costs. The integration of these platforms with the Ayushman Bharat Health Account (ABHA) system is the next frontier, allowing for a seamless flow from consultation to prescription and medicine delivery.
Drone-Led Medical Delivery
In terrains like the Himalayas or the tribal districts of Odisha, terrestrial logistics are often impossible during monsoons or winter. Drones have emerged as a life-saving infrastructure bypass.
Redwing Labs, a Bengaluru-based startup, operates autonomous drone logistics systems to automate last-mile healthcare supply chains. In Odisha's Kandhamal district, Redwing drones transport vital drugs, vaccines, and blood samples across difficult terrains on-demand. These hybrid VTOL (Vertical Take-off and Landing) drones can travel approximately 50 km with a 2 kg payload, reducing replenishment cycles that traditionally took weeks to just a few minutes. Other players like TechEagle and Skye Air Mobility are similarly focused on creating sustainable drone networks for healthcare and agri-commodities, with Skye Air crossing over 20 lakh drone deliveries by late 2025.
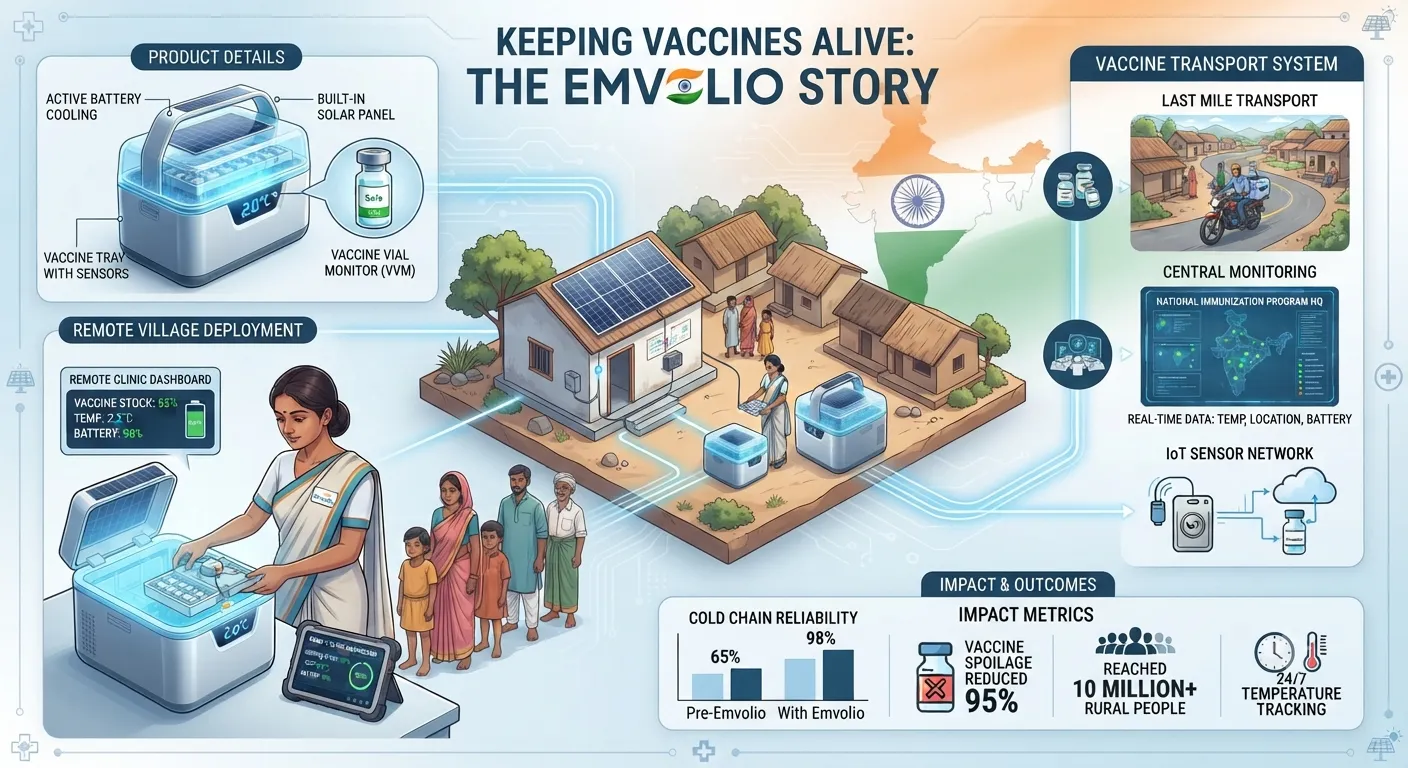
Cold Chain Resilience: The Emvolio Case Study
Vaccine wastage is a critical infrastructure failure, with an estimated 25% of vaccines lost annually in India due to inadequate cold chain management. Traditional iceboxes often fail to maintain the strict 2∘C to 8∘C range required for biologicals, especially in regions with erratic power supply.
Blackfrog Technologies developed Emvolio, a portable, medical-grade refrigerator, to address this specific vulnerability. Emvolio uses solid-state cooling and a precise PID controller to maintain the required temperature for up to 20 hours without the use of ice packs. This eliminates the risk of accidental freezing or thawing—the primary cause of vaccine spoilage in conventional methods. The device is WHO-prequalified, battery-powered, and solar-compatible, making it ideal for the "last-mile" delivery to remote Indian hamlets and even international markets like Kenya and Nigeria. By utilizing an IoT-enabled monitoring system that tracks temperature, humidity, and location, Emvolio provides a level of transparency and traceability that aligns with the goals of the Ayushman Bharat Digital Mission.
Emvolio Impact Metric | Value / Status | Implications | Source |
Vaccine Wastage Reduction | Up to 99% | Drastic cost savings for public health programs. | |
Temperature Range | 2∘C to 8∘C | Precise medical-grade cooling without ice. | |
Operational States (India) | 16 | Proven scalability across diverse climates. | |
Vaccines Delivered | 200,000+ | Direct impact on universal immunization. | |
WHO Certification | Prequalified (Emvolio Plus) | Meets stringent global safety and quality standards. |
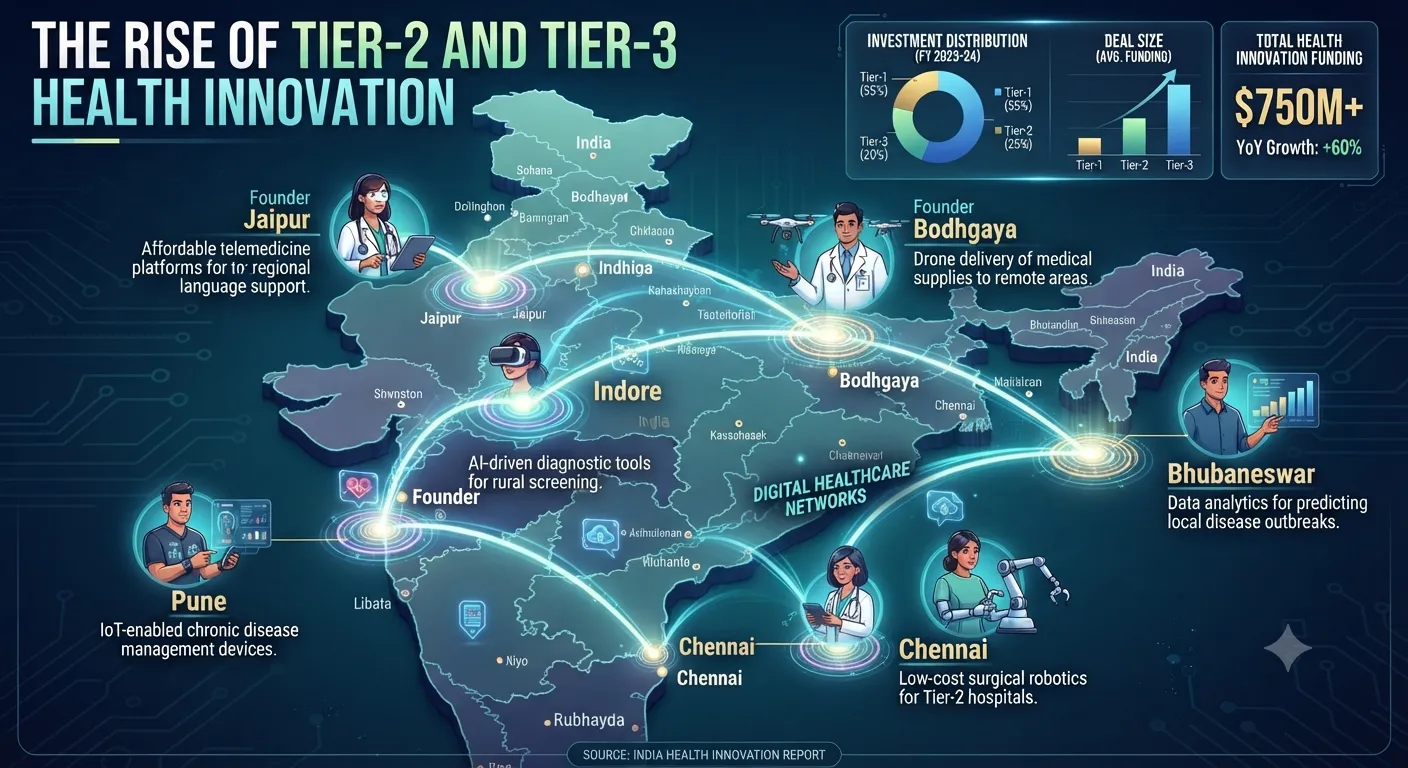
Venture Capital and the Decentralization of Innovation
The Indian HealthTech ecosystem has demonstrated sustained funding momentum despite a moderated startup environment. Between 2014 and 2024, the sector raised approximately $7.25 billion. In 2024 alone, HealthTech startups attracted over $700 million across more than 78 deals, with cumulative funding exceeding $9.9 billion by mid-year.
A significant shift is the decentralization of innovation. Approximately 45% of India’s recognized startups now hail from Tier 2 and Tier 3 cities. These founders are often living among the challenges they solve, such as underserved clinics or erratic supply chains, leading to tailored solutions that resonate in untapped markets. For example, Technoculture Research operates from Bodhgaya and Patna, while Medyseva is based in Indore. This geographic shift is steering India toward a more inclusive era of innovation, where technology is designed for the "raw reality" of the hinterland rather than just the air-conditioned boardrooms of metros.
Notable HealthTech Funding Deals (Late 2025 - Early 2026) | Amount | Round / Investor | Source |
The Eye Foundation | $75.0 M | Late-stage Investment | |
Temple (by Deepinder Goyal) | $54.0 M | First funding round / $190M valuation | |
CureBay | $21.0 M | Series B / Rural infrastructure focus | |
Even Healthcare | $20.0 M | Extended Series A / Alpha Wave Global | |
Nivaan Care | $7.0 M | Series A / Sorin Investments | |
Pulse | $4.0 M | Seed / 3one4 Capital |
Operational Challenges and the Road to Interoperability
Despite the rapid proliferation of technology, several systemic hurdles remain. The adoption of digital health tools is often stalled by a lack of digital literacy among healthcare workers and the high cost of upgrading legacy infrastructure. Interoperability challenges persist because many Indian hospitals still rely on proprietary or standalone IT systems that do not support modern APIs or adhere to standardized clinical terminologies like SNOMED CT.
Furthermore, the introduction of the Digital Personal Data Protection (DPDP) Act has increased the compliance burden for HealthTech startups. Balancing secure data sharing with the need for interoperability remains a core governance challenge. There is also a risk of an "Inequality Loop," where a digital-first architecture may exclude vulnerable groups without smartphones or internet connectivity, potentially weakening trust in the national health system.
The future of Indian HealthTech lies in "Agentic AI" and full interoperability via the ABHA system. By 2026, AI agents are expected to move beyond simple chat functions to coordinating complex tasks like automated billing and real-time insurance processing, which has already shown potential in cutting wait times by 80%. The ultimate goal is to create a seamless health data exchange where records from a wearable, a local lab, and a specialty hospital can "talk" to each other securely, providing a truly longitudinal and portable health record for every citizen.
Synthesis of the HealthTech-Infrastructure Nexus
The emergence of HealthTech startups as primary problem-solvers for Indian infrastructure gaps represents a fundamental shift in the nation's development strategy. Rather than waiting decades for traditional "brick-and-mortar" infrastructure to reach every village, India is utilizing a "Digital Public Infrastructure plus Phygital Delivery" model. This approach leverages the ubiquity of smartphones and the standardization of digital identity (ABHA) to distribute clinical expertise and diagnostic capability across geographies that were previously considered unreachable.
The success of ventures like CureBay in Odisha and Redwing Labs in the Himalayas demonstrates that the rural market is not merely a site for social impact, but a viable, paying consumer base for ethical and efficient healthcare. The integration of AI for mass screening of TB and diabetic retinopathy allows the existing, limited pool of specialists to focus on high-complexity cases, thereby amplifying the "human resource" capacity of the entire country.
In the 2024-2026 period, the focus has shifted from "proof-of-concept" to "operational execution at scale". As startups continue to bridge the gap between urban doctors and rural patients, and as government mandates drive the digitization of private hospitals, the Indian healthcare system is becoming increasingly resilient, data-driven, and equitable. The road ahead requires continued investment in digital literacy and the standardization of data formats, but the momentum toward a unified, technology-led healthcare ecosystem is now irreversible. The combination of indigenous innovation (like Emvolio) and national digital architecture (ABDM) provides a scalable blueprint for other emerging economies facing similar resource constraints and geographic challenges.
Protect Your Future: The Precision Vesting Calculator
Don't let a "handshake deal" complicate your exit. Map out your ownership journey with our Vesting Calculator
Calculate Your Vesting Schedule →